
Imagine some place on Colombia’s Pacific coast: an idyllic riverine community reachable only by boat, where the river is the main road, the rain sets the rhythm of the day, and the sound of the forest blends with the voices of the people. That’s where “María” lives.
One day, during a hospital stay for a cardiovascular condition, she develops a bloodstream infection caused by a multidrug-resistant bacterium. Her hospital does not have ‘Zavicefta’ in stock – that’s a last-line combination antibiotic (ceftazidime–avibactam) designed to treat severe Gram-negative infections that no longer respond to conventional therapy. The outcome for María is painfully predictable: delayed treatment, clinical deterioration, and a narrow window of options disappearing fast.
This scene is not unique to the Colombian Pacific. It could take place in a hospital room in Nairobi, in a district hospital in Dhaka, or in any setting where the geography of antimicrobial resistance and the geography of access fail to overlap. Which, unfortunately, is all too often the case.
This year’s World AMR Awareness Week ended just a few days ago, urging us to “Act now: protect our present, secure our future.” But when it comes to María, and patients in Nairobi, Dhaka, or Port-au-Prince facing the same microbial odds, ‘acting now’ is often impossible for their doctors when the treatments that could protect these patients are simply not available where they are needed.
‘Reserve’
Many of you are probably familiar with the AWaRe Classification of antibiotics, developed in 2017 by the WHO Expert Committee on Selection and Use of Essential Medicines as a tool to support antibiotic stewardship efforts at various levels. In this classification, there are three groups of antibiotics (Access, Watch and Reserve), taking into account the impact of different antibiotics and antibiotic classes on antimicrobial resistance
In the global North, ‘Reserve’ (i.e. last-line antibiotics which WHO aims to preserve for worst case infections) means protecting antibiotics from overuse. In much of the global South, however, ‘Reserve’ refers to the fact that they probably never arrived in the first place. That divide, between who faces the infections and who holds the medicines, is where the double asymmetry begins: a world in which the regions with the heaviest burden have the weakest surveillance, and the least access to the antimicrobials designed for these infections.
Indeed, the burden of multidrug-resistant infections follows a geography of its own, one that rarely overlaps with the geography of resources. The latest (2025) Global Antibiotic Resistance Surveillance Report shows that resistance is often highest in countries with weaker health systems and limited diagnostic capacity. This is echoed in WHO’s assessment of healthcare associated infections’ (HAI) surveillance. If we zoom in on SPAR indicator 9.2 on HAI surveillance (whereby SPAR stands for ‘State Parties Self-Assessment Annual Reporting’ tool on the implementation of the International Health Regulations), according to a recent webinar, Africa’s score has dropped to 35/100, the Americas hover at 56, and the global average has not moved in four years! In many hospitals, the ability to detect an (MDR) outbreak depends less on laboratory infrastructure than on the vigilance of exhausted staff. Put differently, the places where resistant bacteria spread most are the same places least equipped to see them coming.
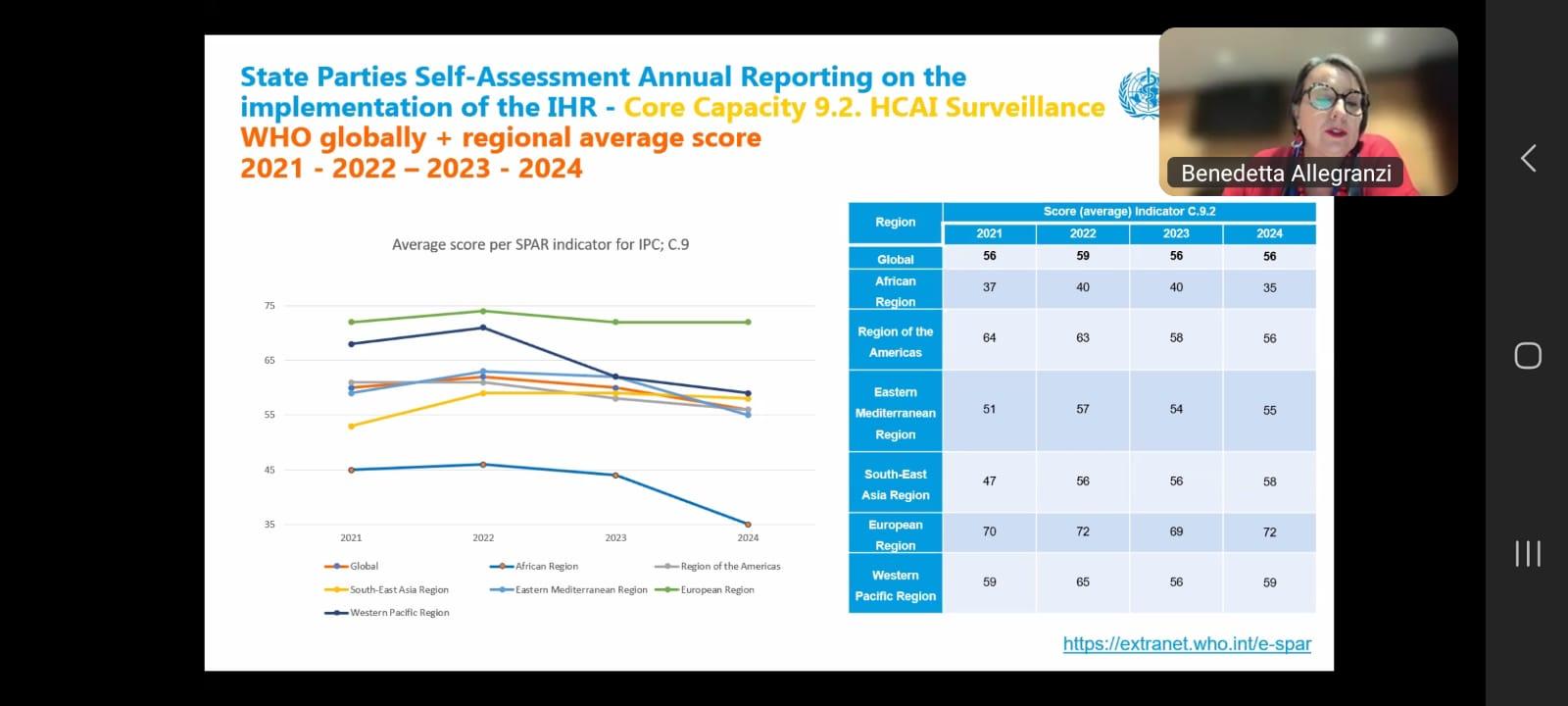
Slide from the webinar, on SPAR indicator 9.2
Last-line antimicrobials are concentrated in the hands of very few actors, and their global distribution reflects that imbalance. As reported in a 2021 Lancet Infectious Diseases article, in 56 of 138 countries the national essential medicines list features not a single ‘Reserve’ antibiotic. And even when these drugs are available somewhere in the supply chain, they rarely reach the bedside. A 2025 multi-country analysis in 8 LMICs found that fewer than 8 % of patients with severe carbapenem-resistant infections received an appropriate antibiotic (and in Kenya, the figure was just 0.2%!).
Time to end the asymmetry
In sum, while much of the global conversation still focuses on restricting the overuse of ‘Reserve’ antibiotics, in a big part of the world they’ve never had the right drug for the right patient at the right time!
Chances are that as long as innovation is rewarded as a private good, access will remain a privilege. We need a model in which new antimicrobials are not only invented, but also guaranteed to reach those who carry the heaviest burden.
Innovation without fair distribution is just another form of inequity.