As health system researchers, how do we contribute to a paradigm shift? How do we move the focus from disease specific/fragmented health programs towards integrated, patient-centred health systems, especially given the abundance of disease-specific funding?
At the recent International AIDS Society conference in Vancouver, Canada I lauded the astonishing achievements of expanding HIV testing, treatment and care for millions of people around the globe. I reflected on the initial reluctance to expanding HIV treatment, especially in Africa. Skeptics cited the lack of infrastructure, funding, multisectoral partnerships and human resources as just a few of the insurmountable barriers. Placing 15 million people on HIV treatment was a result of the combined global efforts of activists, researchers, multilateral organisations, donors, pharmaceutical companies and governments, all of whom were tirelessly battling for decades across sectors and geographical and political lines. They were united by the vision of ending the scourge of HIV/AIDS, refusing to accept the skeptics’ objections. Now it is time for health systems and integrated care to move into the spotlight.
During the IAS conference, strengthening health systems and integrated care were only tangentially mentioned – more as an after dinner mint than a main course or even a dessert. For over a decade international researchers warned of the potential of vertical (i.e., disease specific) HIV programs to fragment weak health systems. International agencies and scholars recommended integrating HIV programmes and focusing on strengthening health systems. However, we lack sufficient evidence on the implementation or “how” to create integrated, people-centred health systems. This is especially true in low and middle income countries.
In March 2015, the World Health Organization (WHO) released the Interim Report of the Global Strategy on People-Centred and Integrated Health Services. Beginning with a need to focus on health system strengthening and the importance of primary health care and universal health coverage, the report discusses how:
“these approaches encourage and support the development of the health system over vertical programming in an effort to provide people with well-planned, integrated health services required to best respond to their health needs across their lifetime and ensure that necessary services reach the most vulnerable”
Five interconnected strategic directions are highlighted as seen below:
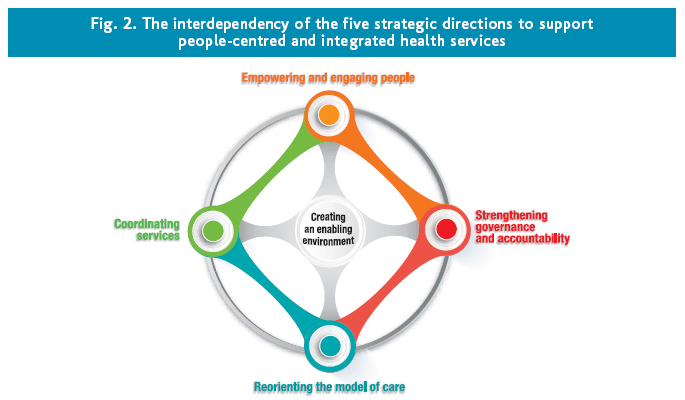
When thinking about “how” to shift the paradigm towards people-centred and integrated health services many challenges exist. These challenges are related to systems, people, organisations and leadership. As summarised in the report, empowering patients, families and communities to become more involved in health care decision making questions the existing medicalised model of health systems (i.e., where medically trained health providers are the sole decision makers). System related challenges include changing organisational, legal, governance and accountability structures within health systems. Disease specific funding and targets within health systems limit intersectoral collaboration. People related challenges include encouraging inter-disciplinarity between professional groups while maintaining patients and communities as equal partners in health care. Organisational- related challenges include the alignment and management of diverse values and goals across regional governing bodies, non-profit organisations and the private sector. Leadership related challenges exist at and within country levels that necessitate models of distributed leadership as people-centred and integrated health services will need to be tailored to local needs.
Many of these challenges are reminiscent of the early dialogue around why a global HIV/AIDS response could not be successful, especially in low and middle income countries. What can we learn from the global HIV response and the related paradigm shift? Researchers, activists, communities, and patients refused to accept that improving access to HIV treatment was impossible, producing evidence and action to bolster this. Likewise, we should not accept that shifting a paradigm towards patient-centred, integrated health systems is impossible. We must recognise the evidence gaps, especially those related to implementation science and challenge our institutions and governments to fill them. We must prioritize health systems research that engages patients and communities to ensure their needs are met. We must develop, test, share and refine metrics of patient and community engagement and integrated service delivery in health systems research. We must bridge across disciplines and sectors to arrive at cost-effective solutions that prioritise patients.
Why is it no longer acceptable to die at the hands of a virus like HIV but is it still considered acceptable to die due to modifiable health system factors? The time to change is now. Our health systems can and should meet the needs of patients and communities. So let’s get started.