Forty years after the well-intentioned Alma Ata Declaration (1978), ‘Health for All’ remains a distant goal. This is particularly so for populations living in vulnerable parts of the world – conflict areas, prone to natural disasters, or geographically remote and vulnerable areas such as the Sundarbans in India. How does one, in the era of the SDGs ensure that goal #3 is achieved for the most marginalized? This blog takes us to the riverine areas of the Sundarbans in India to understand better the contextual factors which inhibit the provision, and access to health services for the people living there.
The Sundarbans is one of the largest mangrove forests in the world. Located along the Bay of Bengal the forest spans Bangladesh and India. It is a mix of tidal waterways, mangrove forests, and mudflats. While the area might hold the status of a UNESCO World Heritage Site, it is challenged by poor availability and access to social and development services. In addition, the unique geographical composition of the region makes it vulnerable to climate change, abject poverty, and the threat of uncontrolled commercialization.
The remote and often difficult to access geographical setting of the Sundarbans makes the provision of health and other social services a challenge. In addition, socio-cultural factors (caste, religion and gender), and economic constraints pose as significant barriers in access to health services.
A child born in this region is likely to be at a disadvantage from birth, affected (in all likelihood) by the poor health and nutritional status of the mother at the time of conception and gestation, to its birth. Limited access to health facilities, or skilled birth attendants, and health services put the mother and infant at risk. Socio-cultural contexts and the economic status of the household a child is born into would further impact access to education, nutrition and other opportunities of a child born in this region. Girls often drop out of school to take care of younger siblings while women try and secure a livelihood. Women in the region are also vulnerable to trafficking. Boys too are likely to drop out of school at a young age to join the older men of the community in towns and cities as migrant workers.
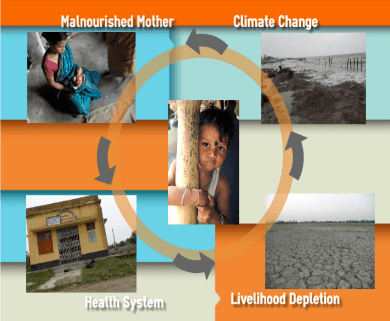
Fig 1 – Source: International Institute Of Health Management Research University
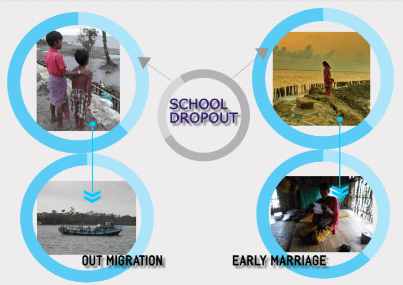
Fig2: Source: International Institute Of Health Management Research University
Within such a context the question arises to what extent the provision of even pro-poor health services would be beneficial to people living in marginalized settings, if contextual forces (such as climate impact, livelihood scarcity or food insecurity) are not addressed? The situation demands comprehensive strategies and a conscious, collective effort to address not only physical challenges of delivering health services, but also simultaneously tackling the wider social determinants of health.
UHC is put forward by Dr Tedros as his core objective. We hope the issues of context – social, cultural, economic, and geographic ones, among others – will not be overlooked. Achieving UHC requires broad collective action on health, with an effort to be more inclusive, and with more effective inter-sectoral collaboration. Strengthening the health system, particularly the existing public health system and enhancing human resources for health, as well as tackling issues of poverty, livelihood, and education will be critical towards achieving health and social development indicators. Political will and effective governance are also critical towards health system strengthening. Effective coordination between local stakeholders and higher-level stakeholders will be vital to health care delivery.