
The 79th World Health Assembly (WHA) convened in Geneva against a backdrop of the Declaration of a Public Health Emergency of International Concern (PHEIC), a global health financing crisis, geopolitical fracture, and urgent calls for systemic reform. This article surveys the key decisions and debates — and asks whether the WHA’s outcomes will deliver the human rights-grounded global health governance the moment demands. It draws on input from WHA first-timer Valérie Vermeersch and seasoned WHA attendee Rachel Hammonds.
Geneva in a Fractured World
The roadwork wasn’t the only thing rerouting Geneva. WHA79 took place at a moment of acute strain in global health governance and multilateralism more generally. The United States, historically among the most influential countries at the WHA, remained conspicuously absent from key negotiations, a geopolitical and financial void that shaped the dynamics of nearly every major agenda item. Against this backdrop, Ghana, a country advancing health rights through implementing free access to primary health care, along with other African member states played an unusually prominent role, stepping into spaces left by Washington’s retreat and articulating a vision of health governance grounded in sovereignty, alignment, equity and solidarity.

Getting to the Intercontinental from Global Fund or the Palais was challenging.
Global Health Architecture Reform: Process Without Promise?
Credit where it’s due to the ever-present, relentless Accra Reset team, led by President John Mahama, whose in-person presence left no doubts over his commitment to lead and deliver on what country-led delivery requires in practice at the national, regional and global levels. In contrast the WHA decision to establish a joint, Member State-led process – hosted by WHO – has led to serious questions about where the WHA reform process will really lead — and who will drive it.
But process and promises are different from progress and all reform must deliver. A vocal Kenyan civil society representative at the Accra Reset Geneva Clarion Call side event rejected the Kenyan Cabinet Secretary for Health’s claims about Kenya’s progress on expanding access to Universal Health Coverage (UHC). Her frustration highlights the necessity of rapidly delivering on progress, not just talking about it.
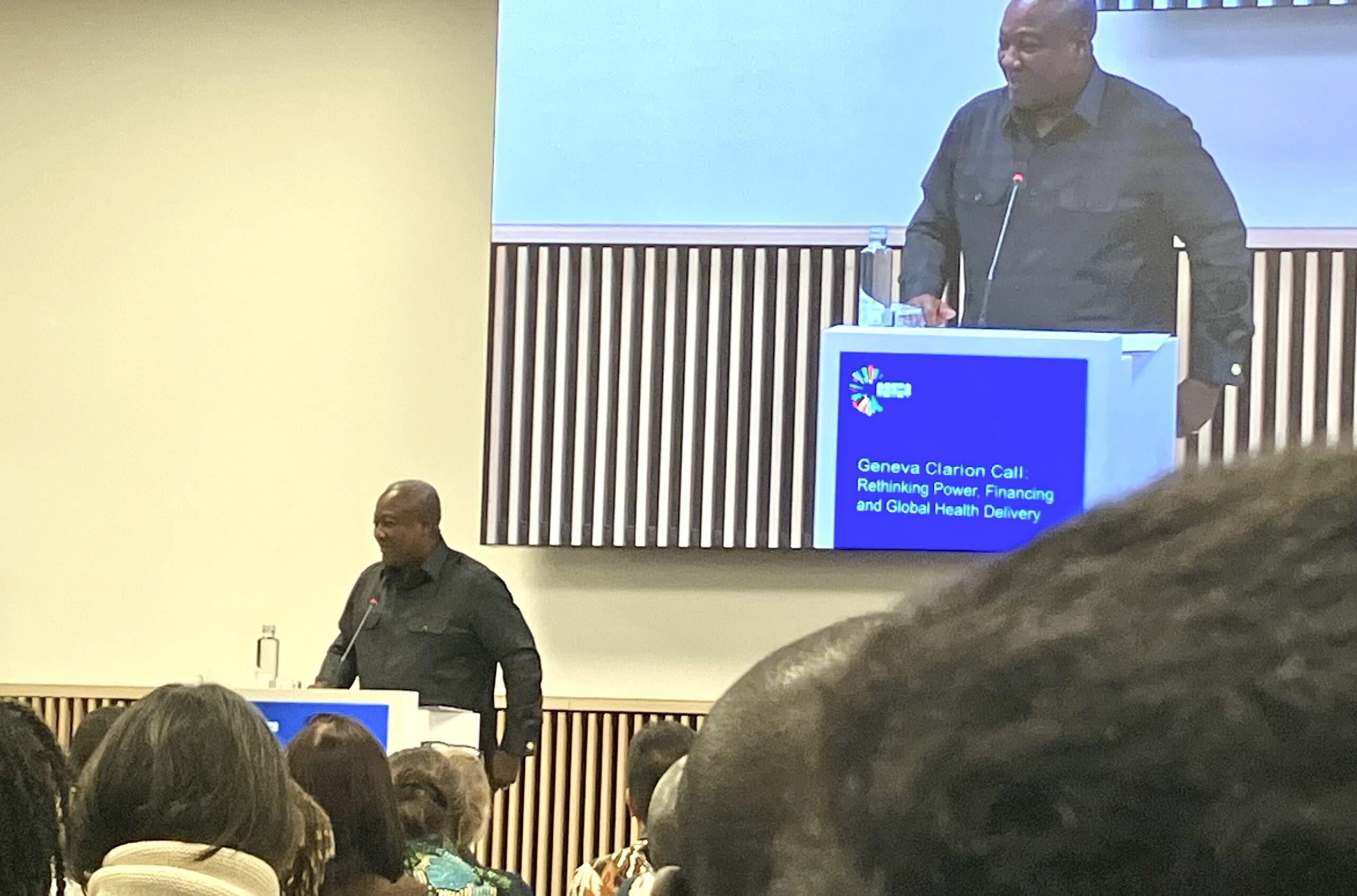
The Ghana president at the Clarion call event
Digital health and AI featured prominently across reform discussions framed, repeatedly, as a transformative solution to address health systems challenges and financing gaps. There is genuine potential here: digital tools can extend reach, improve data, and enable more responsive care and self-care. But, as the Digital Health and Rights Project emphasised, unless digital solutions engage with the structural drivers of health inequity and rights denial they risk replicating existing injustice. The critical question is whether reform processes will be anchored in rights-based frameworks — or whether they will be captured by efficiency, technical solutions and financing logics that sideline accountability, participation, and non-discrimination.
Civil society observers, including the People’s Health Movement, have been clear: ‘structural reform’ without rights is restructuring without justice.
Health as Investment: WHO’s Economics of Health for All (EHA) Strategy (2026-2030)
The new Strategy aims to align economic systems with health, equity, and sustainable development. The Strategy marks a genuine shift in WHO’s economic framing, moving away from a purely cost-minimisation logic toward one that treats health expenditure as productive investment. But critics, including civil society organisations present at WHA, warn that the Strategy subordinates the original focus on investment, rights and equity in the WHO Council on the Economics of Health For All, to investment. David McCoy of United Nations University highlighted the increasing financialisaton of health – concentrating economic power in private hands at the expense of states- and stressed the need for safeguards to protect health equity.
Ensuring health as a human right is not contingent on its economic returns. As UN High Commissioner for Human Rights, Volker Turk and WHO DG Tedros have made clear, ¨All national economic, fiscal, monetary, investment and business decisions should be viewed, and managed, through the lens of health and human rights.” Where investment logic dominates, the populations whose health yield the lowest measurable economic dividend – the poorest, the most marginalised – are at greatest risk of being deprioritised. The elements of a rights-based approach – social participation, equity – may be present in the Strategy’s text, but the accountability mechanisms and binding standards integral to the UN human rights system are largely absent.

Sexual and reproductive health and rights (SRHR): The Silence That Speaks Volumes
SRHR, gender equality and women’s rights took up little space on the formal agenda at WHA79, a silence that is itself politically significant. The human impact of funding cuts on progress on maternal and child health commitments and the urgency of progress was stressed by Helen Clark at a Partnership for Maternal, Newborn and Child Health Lives in the Balance Event. As the BMJ’s Jocelyn Clark and others have observed, the marginalisation of SRHR and gender in multilateral health spaces reflects the same political pressures that have made them a target in domestic policy contexts across the globe.
Climate and Health: Fossil Fuels in the Frame
An increasing focus on climate justice and the intersection of climate change and global health provides a glimmer of hope. The recent, non-binding International Court of Justice (ICJ) advisory opinion on states’ climate obligations demonstrates the power of collective action to drive change. A youth representative and some Small Island Developing States (SIDS) representatives- which bear the least responsibility for climate change while facing its most severe consequences – were joined by Sunway Centre for planetary health’s Dr Jemilah Mahmood and WHO Legal Counsel to explore how the ICJ opinion represents a potential legal lever for demanding accountability from major emitters. The energy of the youth delegates and the motivation of SIDS leaders, whose countries and culture already face an existential threat, signalled a growing appetite to bring fossil fuel accountability directly into the global health governance frame.
Trust in crisis: how to rebuild trust into the system?
Across numerous side events, a recurring challenge emerged as central to global health architecture reform, implementation of the Pandemic Agreement and difficult Pathogen Access and Benefit Sharing (PABS) annex negotiations: a deep and widening lack of trust, including strained trust between Member States, between public and private actors, and more broadly in multilateralism itself (by some countries).
But the crisis of trust extends beyond diplomatic negotiating rooms. At community level, mistrust in Ministries of Health and other public health institutions has deepened, fuelled by the rapid circulation of misinformation and disinformation through social media ecosystems, as well as by tensions between health priorities and competing societal values. A recent example from the Democratic Republic of Congo, where Ebola treatment tents were set on fire by an angry crowd, illustrates how rapidly fear, misinformation and perceived exclusion can translate into violence against health infrastructure itself.
Thus, rebuilding trust emerges as a critical precondition for meaningful reform at all levels of the global health system.
PABS at WHA79: Absent from the Table, Present in many Rooms
PABS was notably absent from substantive discussion at WHA79, as Member States had not reached agreement ahead of the Assembly, despite this having been the stated ambition. At the World Health Assembly, MS just supported the extension of talks on PABS. In side events, however, it was still occasionally referenced in broad and indirect terms within wider debates on equity, trust, and global health security rather than as a technical negotiation item (only). These references reflect the numerous unresolved tensions at the heart of pandemic preparedness.
More broadly, they point to a persistent trust deficit between countries (among others western and low-and middle-income countries) and ongoing questions about the legitimacy of multilateral approaches to shared health threats. The work continues in the Intergovernmental Working Group (IGWG) (which reconvenes in July), but attention is also shifting now to the United Nations General Assembly high-level meeting on pandemic prevention, preparedness and response in September, where PABS may re-emerge more explicitly in the discussions.
Conclusion: Reform Needs To Rebuild Trust and Deliver Rights
WHA79 was productive. Decisions were taken on advancing architecture reform and health economics. And yet a thread runs through all these debates: the risk that reform processes driven by financing imperatives, geopolitical compromise, and institutional incrementalism will produce a global health architecture that is more efficient, less costly but no more just.
Ultimately, without rebuilding trust – between states, institutions, and communities – no reform process will be able to deliver a rights-based, equitable global health governance.

The two authors at the lake in Geneva