
The global healthcare landscape is currently witnessing a digital renaissance. Across Low- and Middle-Income Countries (LMICs), the acceleration of telehealth, AI-enabled diagnostics, and national digital health missions—aligned with the WHO Global Strategy on Digital Health 2020–2027—promises a future where geography no longer dictates the quality of care.
However, beneath the veneer of high-tech progress lies a sobering reality. As we lean into the “digital first” era in countries like mine (India), we risk building sophisticated systems that many staff on the frontline find hard to navigate. With all the implications you can imagine for vulnerable populations (including those who are digitally excluded, linguistically marginalized, economically constrained, or culturally overlooked—and more in general, those who lack agency in shaping the tools, policies, and systems that govern their care).
If digital adoption continues to outpace digital and health literacy, as cautioned in the OECD Health at a Glance 2025 projections, we aren’t just “improving” systems. Unfortunately, we will also be creating new, invisible layers of exclusion.
Lessons from the Frontline: The Software Struggle
The implementation gap is not merely a theoretical concern; it is a daily reality for healthcare professionals. During my work within a multispecialty hospital network in India, I witnessed firsthand the friction between advanced digital tools and clinical workflows.
Despite the high-stakes nature of a hospital setting, highly skilled professionals—doctors, embryologists, nurses, and clinic managers—consistently struggled with the specialized software designed to streamline their work. We found that even “minute functions” became hurdles, consuming cognitive energy that should have been reserved for patient care. When a nurse is battling an interface to log a vital sign, or an embryologist finds a data-entry field counterintuitive, the software is no longer a tool: it is a barrier.
This experience underscores that even in specialized, urban healthcare settings, digital adoption without empathetic, strategic communication leads to burnout and inefficiency. This friction is not anecdotal: recent findings confirm that even specialized clinicians report a significant “cognitive load” when digital tools are not aligned with existing clinical workflows.
Beyond the “Soft Skill” Fallacy
In the traditional development of health technology, communication is often relegated to the final stages of a project—a peripheral “soft skill” used for marketing or user manuals. This is a fundamental governance failure.
According to the WHO Strategic Communications Framework (for effective communication), communication is a core function. In the context of digital health, it is the mechanism that determines:
The Tension Between Strategy and Reality
Current global digital health ambitions often focus on “scalability” and “interoperability”—technical milestones that look excellent in policy briefs. Yet, the implementation gap in LMICs remains wide because high-level strategies frequently overlook the local realities of the end-users who are healthcare providers.
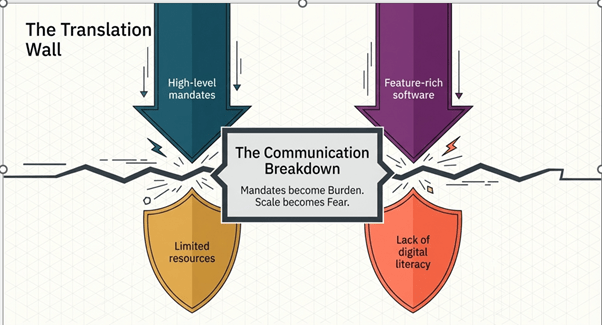
Image: 1- The Anatomy of Digital Friction
Image 1 shows that while each stakeholder in digital health has a valid goal, a variety of communication gaps prevent alignment and effective implementation. Policymakers overlook local context, tech solutions alienate users, frontline workers see tools as burdens, and communities struggle with trust and literacy. Ultimately, the challenge is not intent, but the lack of a shared, inclusive communication framework connecting all stakeholders.
This gap is increasingly documented in the literature. For instance, a 2025 Frontiers in Digital Health review identifies a critical ‘mismatch’ between developer expectations and the lived reality of health workers, suggesting that technical scalability means little if it ignores the cognitive load of the user.
Integration from the Start: A New Digital Health Governance Model
To ensure that the digital revolution does not leave people on the frontline behind, we must pivot. Digital health governance must integrate strategic communication and literacy planning from the very first line of code.
A Call to Action
As we evaluate the progress of global health initiatives, the message for the international medical community is clear: the digital divide is not just about who has a smartphone; it is also about who has a voice in how those tools are designed.
We must champion a model whereby “innovation” is measured not by the complexity of the algorithm, but by the clarity of the connection between the system and the human(s) it serves.
Digital health can truly democratize medicine—but only when communication is no longer treated as an afterthought and instead becomes the foundation of inclusive, people-centered governance.