Over the last years there has been much research on and proposals for governance in health systems whether at the district, national or global level. Since mid-nineties or so there have been reforms in countries to initiate public- private cooperation, e.g. via the contracting of health service delivery. At global level, there has been debate about the development and impact of public private health initiatives such as GAVI which was launched at the World Economic Forum in 2000
More recently, there has been attention for health policies based on intersectoral collaboration and multistakeholder processes. They are presented as key to overcome health problems in our globalized societies. Francis Fukuyama asked in The End of History? whether there are viable alternatives to the model of western liberal policies, based on individual freedom, human rights and a capitalist democracy. Many modern health governance policies build forward on this idea, and propose frameworks that besides the state include multiple non-state actors, that each on their individual merit (civil society, academia, philanthropy, labor unions, patient groups, business corporations etc.) deserve to be included in health policy development.
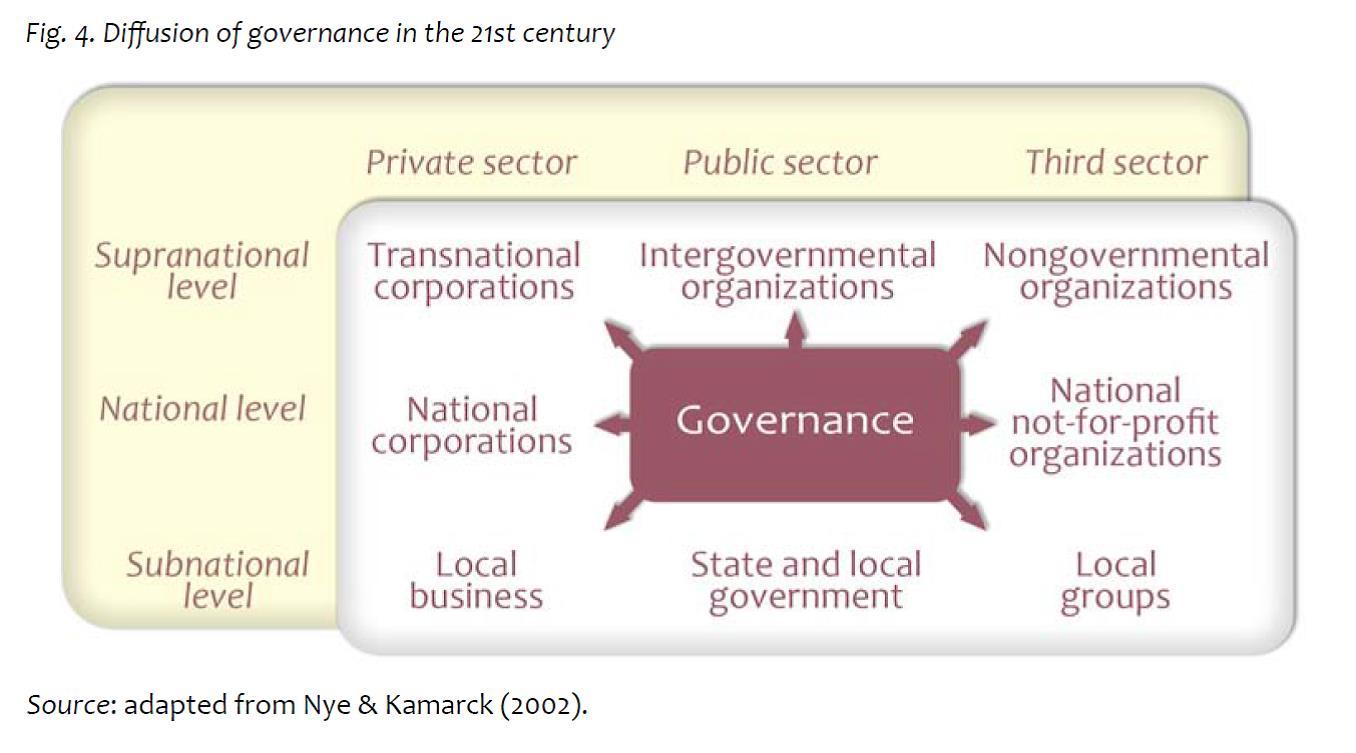
Ilona Kickbush’sGovernance for Health in the 21st century provides a detailed overview over these developments, and explains how a whole-of-society and a whole-of-governance approach is required to enhance health equity. Health is a co-creation by many actors in society, and hence there should be a diffusion of governance at different policy levels to make this happen.
UNDP provides the following definition:
“ The aim of multistakeholder processes are to promote better decision making by ensuring that the views of the main actors concerned about a particular decision are heard and integrated at all stages through dialogue and consensus building. The process takes the view that everyone involved in the process has a valid view and relevant knowledge and experience to bring to the decision making. The approach aims to create trust between the actors and solutions that provide mutual benefits (win-win). The approach is people-centered and everyone involved takes responsibility for the outcome…”
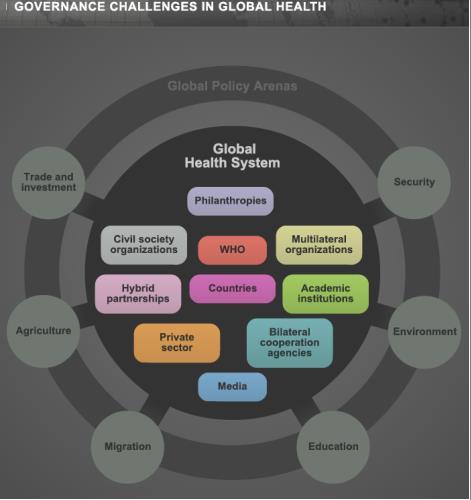
At global level there has been a push for multiple stakeholder mechanisms, and to have the state-centered multilateral UN agencies reform as to engage other actors in global health governance (see the figure below). In many institutions including the Global Fund (to fight against AIDS, Tuberculosis and Malaria), GAVI and very likely also in a new Global Coordination Mechanism on NCDs, non-state (or perhaps better non-government) actors have a board position and/or are included in the policy dialogue and agenda setting. However, within the World Health Organization there is still no consensus on a policy framework for cooperation with non-state actors.
There have been positive cases and enthusiast examples about these new innovative models to address modern health problems. These examples include Communities of Practice on Harmonization for Health in Africa, the Health–in-All Policies approaches in South-Australia & Finland and the National Health Assembly in Thailand.
But there are critical voices as well. Researchers assess a potential undermining of the public interest in health and warn us of the political determination within these new governance arrangements. Even Margaret Chan, WHO’s DG stated in June 2013:
“When industry is involved in policy-making, rest assured that the most effective control measures will be downplayed or left out entirely. This, too, is well documented, and dangerous. In the view of WHO, the formulation of health policies must be protected from distortion by commercial or vested interests.”
At global level, many frameworks have been recently proposed including a non-state centric governance model for global health, a framework convention on global health , to split the WHO in two distinctive parts but also a more state-centred approach to address global health inequalities via supranational mechanisms to enforce rights, redistribution and regulation.
We encourage the readers to provide us with examples, experiences and critical reflections on multistakeholder processes for health at (sub)national or global levels. The thematic area (e.g. health financing, access to medicines, tobacco control) or disease focus (e.g. HIV/AIDS, NCDs, Neglected Tropical Diseases) is flexible, depending on the author’s expertise.
Contributions can be guided by questions like:
Contributions should be around 700-800 words and to be submitted before 15th of September 2014.
The blogs will be published in a special edition of the IHP newsletter focused on governance for health in October 2014.
For questions, remarks and submissions contact rvandepas@itg.be.